AI Generated Quiz
A Level H2 Biology Human Physiology Quiz
Free A Level H2 Biology Human Physiology quiz, LongCat AI version, with questions, answers, and A Level-style practice for Singapore students.
These static practice materials are generated from the site's syllabus and paper-generation workflow, with source and model context shown so students and parents can evaluate the material before use.
Questions
A-Level Biology H2 Quiz - Human Physiology
Name: ___________________________
Class: ___________________________
Date: ___________________________
Score: ________ / 60
Duration: 60 minutes
Total Marks: 60
Instructions:
- Answer ALL questions in the spaces provided.
- The number of marks for each question is shown in brackets [ ].
- Where a question requires explanation or description, answers should be written in continuous prose with correct scientific terminology.
- Where data interpretation is required, refer clearly to the figure or data provided.
- The total marks for this paper is 60.
Section A: Multiple Choice Questions [10 marks]
Questions 1–10 carry 1 mark each. Choose the single best answer.
1. Which of the following correctly describes the role of the sinoatrial node (SAN) in the cardiac cycle?
A. It delays the electrical impulse to allow ventricular filling.
B. It acts as the pacemaker, initiating the electrical impulse that spreads across the atria.
C. It conducts impulses directly from the atria to the ventricles.
D. It generates the highest pressure during ventricular systole.
[1]
2. During the sliding filament model of muscle contraction, which molecule directly provides the energy required for the myosin head to detach from actin?
A. ADP
B. ATP
C. Creatine phosphate
D. GTP
[1]
3. A person with Type I diabetes mellitus is unable to produce sufficient insulin. Which of the following best describes the expected blood glucose profile after a carbohydrate-rich meal compared to a healthy individual?
A. Blood glucose rises more slowly and returns to normal faster.
B. Blood glucose rises to a higher level and remains elevated for longer.
C. Blood glucose does not rise at all because glucose cannot be absorbed.
D. Blood glucose rises normally but falls below normal due to excess glucagon.
[1]
4. Which of the following correctly describes the mechanism of action of steroid hormones?
A. They bind to cell surface receptors and activate a second messenger cascade.
B. They diffuse across the plasma membrane and bind to intracellular receptors to regulate gene transcription.
C. They activate G-protein coupled receptors on the cell surface.
D. They are transported into the cell via facilitated diffusion and bind to membrane-bound enzymes.
[1]
5. In the nephron, the majority of glucose reabsorption occurs in which region?
A. Distal convoluted tubule
B. Loop of Henle
C. Proximal convoluted tubule
D. Collecting duct
[1]
6. Which of the following best explains why the resting membrane potential of a neurone is approximately −70 mV?
A. The sodium-potassium pump actively transports equal numbers of Na⁺ and K⁺ across the membrane.
B. The membrane is more permeable to Na⁺ than K⁺ at rest.
C. The membrane is more permeable to K⁺ than Na⁺ at rest, and the sodium-potassium pump maintains ion gradients.
D. Chloride ions accumulate inside the cell, making the interior negative.
[1]
7. During an inflammatory response, histamine is released by mast cells. What is the primary effect of histamine on blood capillaries?
A. Vasoconstriction and decreased permeability
B. Vasodilation and increased permeability
C. Activation of complement proteins
D. Stimulation of antibody production by B lymphocytes
[1]
8. Which of the following correctly describes the role of surfactant in the alveoli?
A. It increases surface tension to prevent alveolar collapse.
B. It decreases surface tension to prevent alveolar collapse during expiration.
C. It transports oxygen across the alveolar epithelium.
D. It stimulates the contraction of the diaphragm during inspiration.
[1]
9. In the control of osmoregulation, osmoreceptors are located in the:
A. Posterior pituitary gland
B. Adrenal cortex
C. Hypothalamus
D. Collecting duct of the nephron
[1]
10. Which type of T lymphocyte is responsible for directly killing virus-infected cells?
A. Helper T cells (CD4⁺)
B. Cytotoxic T cells (CD8⁺)
C. Regulatory T cells
D. Memory T cells
[1]
Section B: Structured Questions [30 marks]
Questions 11–16 carry varying marks. Answer in the spaces provided.
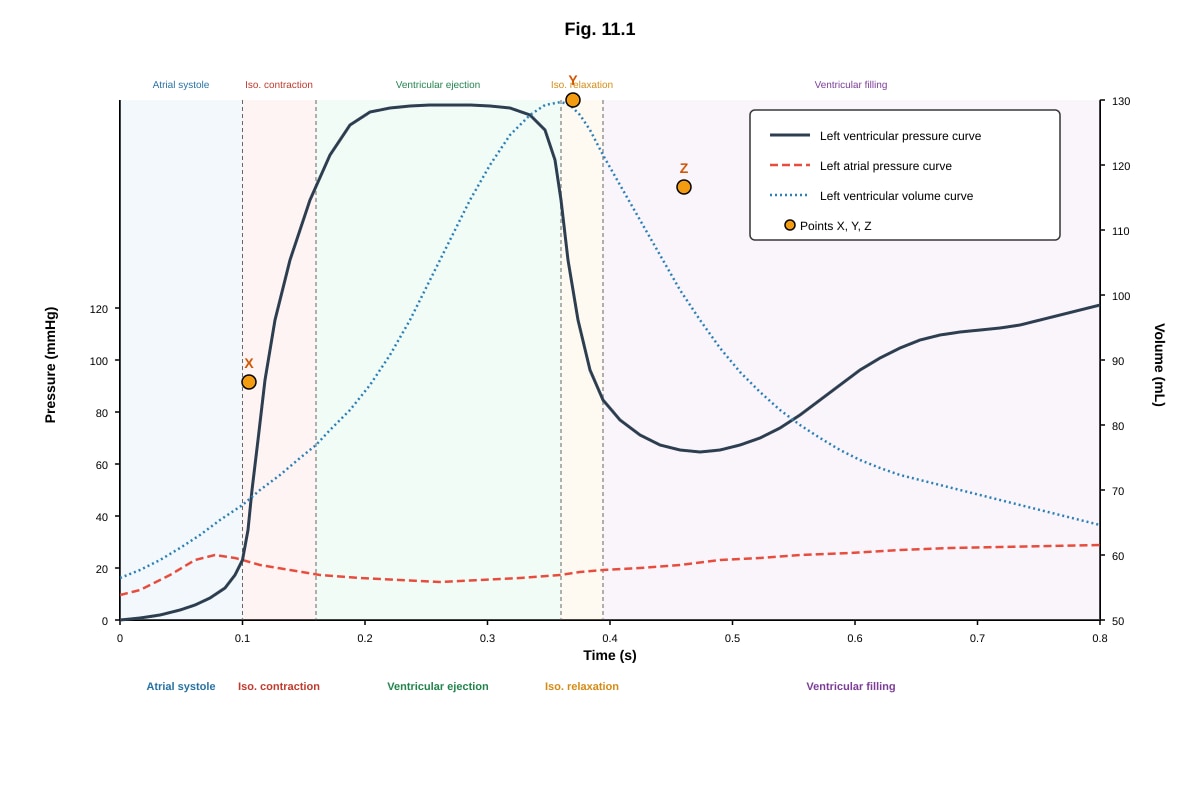
11. Fig. 11.1 shows the changes in pressure and volume in the left side of the heart during one cardiac cycle.
Generated graph for Q11.
(a) With reference to Fig. 11.1, state the time at which the atrioventricular (AV) valve closes. Explain your answer. [2]
(b) Explain the pressure changes occurring in the left ventricle between points X and Y. [3]
(c) Describe the events occurring in the cardiac cycle between points Y and Z. [3]
[8]
12. (a) Describe the sequence of events that occurs at a neuromuscular junction when an action potential arrives at the axon terminal of a motor neurone. [4]
(b) Explain how the sliding filament theory accounts for muscle contraction, including the roles of calcium ions, ATP, and the proteins actin and myosin. [5]
[9]
13. Table 13.1 shows the concentrations of various substances in blood plasma, glomerular filtrate, and urine in a healthy human.
| Substance | Blood Plasma (g/100 cm³) | Glomerular Filtrate (g/100 cm³) | Urine (g/100 cm³) |
|---|---|---|---|
| Water | 90–93 | 90–93 | 95–97 |
| Protein | 7.0–8.0 | 0.0 | 0.0 |
| Glucose | 0.10 | 0.10 | 0.00 |
| Urea | 0.03 | 0.03 | 2.00 |
| Sodium ions | 0.32 | 0.32 | 0.60 |
| Chloride ions | 0.37 | 0.37 | 0.60 |
(a) Explain why protein is present in blood plasma but absent in the glomerular filtrate. [2]
(b) Explain why glucose is present in the glomerular filtrate but absent in the urine of a healthy person. [2]
(c) The concentration of urea in urine is approximately 67 times that in blood plasma. Explain this observation. [2]
(d) Suggest why the concentration of sodium ions in urine is higher than in blood plasma, even though sodium ions are actively reabsorbed in the nephron. [2]
[8]
14. (a) Distinguish between innate immunity and adaptive immunity. [3]
(b) Describe the process of clonal selection and clonal expansion during a humoral immune response. [4]
[7]
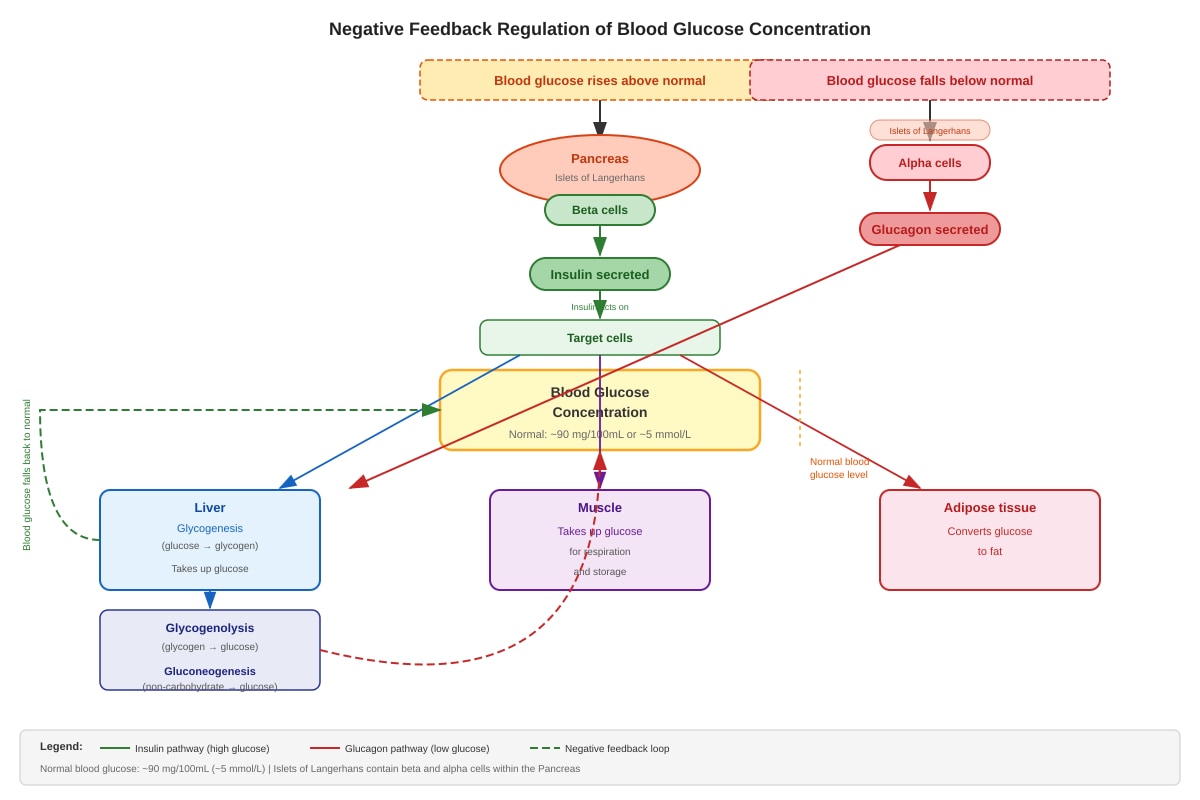
15. Fig. 15.1 shows a negative feedback loop involved in the regulation of blood glucose concentration.
Generated diagram for Q15.
(a) With reference to Fig. 15.1, state two ways in which insulin lowers blood glucose concentration. [2]
(b) Explain why the regulation of blood glucose is described as a negative feedback mechanism. [2]
(c) A patient is diagnosed with Type II diabetes mellitus. Explain how insulin resistance in target cells leads to persistently elevated blood glucose levels. [3]
[7]
16. (a) Describe the role of the hypothalamus in thermoregulation in humans. [4]
(b) Explain how the body responds to a decrease in core body temperature, including the roles of vasoconstriction, shivering, and the metabolic response. [4]
[8]
Section C: Free Response Questions [20 marks]
Questions 17–20 carry varying marks. Answer in the spaces provided.
17. Describe the transmission of an action potential along a myelinated neurone. In your answer, explain the roles of voltage-gated sodium channels, voltage-gated potassium channels, and the myelin sheath in the propagation of the nerve impulse. [8]
[8]
18. Explain how the human body maintains blood pH within a narrow range (pH 7.35–7.45). In your answer, include the roles of the carbonic acid–hydrogen carbonate buffer system, the respiratory system, and the kidneys. [7]
[7]
19. Compare and contrast the humoral and cell-mediated immune responses. In your answer, include the types of cells involved, the targets of each response, and the mechanisms by which pathogens are eliminated. [5]
[5]
20. A student carried out an investigation into the effect of exercise on heart rate and breathing rate. The results are shown in Table 20.1.
| Time (min) | Resting (0–2) | Exercise (2–10) | Recovery (10–15) |
|---|---|---|---|
| Heart rate (beats/min) | 72 | 155 | 78 |
| Breathing rate (breaths/min) | 14 | 32 | 16 |
| Tidal volume (mL) | 500 | 2500 | 550 |
(a) Calculate the cardiac output (in L/min) of the student during exercise. Show your working. [2]
(b) Explain the physiological changes that cause the increase in heart rate and breathing rate during exercise. [4]
(c) Explain why heart rate and breathing rate do not immediately return to resting values when exercise stops. [3]
[9]
Answers
A-Level Biology H2 Quiz - Human Physiology
Answer Key and Marking Scheme
Section A: Multiple Choice Questions [10 marks]
1. B
Marking: 1 mark for B only.
Explanation: The sinoatrial node (SAN), located in the right atrial wall, is the natural pacemaker of the heart. It spontaneously generates electrical impulses that spread across the atria, causing atrial contraction. Option A describes the AV node; option C describes the Bundle of His/Purkinje fibres; option D is incorrect as the SAN does not generate pressure.
2. B
Marking: 1 mark for B only.
Explanation: ATP binds to the myosin head, causing it to detach from the actin filament. Hydrolysis of ATP to ADP + Pᵢ then provides the energy to "re-cock" the myosin head into its high-energy conformation, ready for the next power stroke. Without ATP, myosin remains bound to actin (rigor state).
3. B
Marking: 1 mark for B only.
Explanation: In Type I diabetes, insufficient insulin means that glucose uptake by target cells (liver, muscle, adipose) is impaired, and glycogenesis is reduced. After a carbohydrate-rich meal, blood glucose rises to a higher level than normal and remains elevated for longer because the negative feedback loop involving insulin is defective. Option D describes hypoglycaemia, which is not the primary consequence.
4. B
Marking: 1 mark for B only.
Explanation: Steroid hormones (e.g., cortisol, oestrogen, testosterone) are lipid-soluble and diffuse freely across the plasma membrane. They bind to intracellular receptors (often in the nucleus) to form a hormone-receptor complex that acts as a transcription factor, regulating gene expression. Option A describes peptide hormones; option C also describes peptide hormone mechanisms.
5. C
Marking: 1 mark for C only.
Explanation: The proximal convoluted tubule (PCT) is the site of the majority of selective reabsorption. Glucose is reabsorbed here by active transport (co-transport with Na⁺ via SGLT transporters) and facilitated diffusion (GLUT transporters). In a healthy person, virtually 100% of filtered glucose is reabsorbed in the PCT.
6. C
Marking: 1 mark for C only.
Explanation: At rest, the neurone membrane is more permeable to K⁺ than Na⁺ due to open K⁺ leak channels. K⁺ diffuses out of the cell down its concentration gradient, making the interior more negative. The sodium-potassium pump (3 Na⁺ out, 2 K⁺ in per ATP) maintains the concentration gradients and contributes directly to the negative potential (electrogenic effect). Option A is incorrect because the pump is electrogenic (unequal ion exchange).
7. B
Marking: 1 mark for B only.
Explanation: Histamine causes vasodilation (widening of blood capillaries) and increased capillary permeability, allowing plasma proteins and phagocytes to move into the infected tissue. This produces the characteristic redness, heat, and swelling of inflammation.
8. B
Marking: 1 mark for B only.
Explanation: Surfactant, secreted by Type II alveolar cells, reduces the surface tension of the fluid lining the alveoli. This prevents alveolar collapse (atelectasis) during expiration when alveolar volume decreases. Without surfactant, the surface tension would increase as alveoli shrink, causing them to collapse.
9. C
Marking: 1 mark for C only.
Explanation: Osmoreceptors in the hypothalamus detect changes in water potential (osmolarity) of the blood. When blood water potential decreases (becomes more concentrated), the osmoreceptors stimulate the posterior pituitary to release antidiuretic hormone (ADH), which increases water reabsorption in the collecting ducts.
10. B
Marking: 1 mark for B only.
Explanation: Cytotoxic T cells (CD8⁺) recognise antigens presented on MHC class I molecules on the surface of virus-infected or cancerous cells. They kill these cells by releasing perforin (which forms pores in the target cell membrane) and granzymes (which trigger apoptosis). Helper T cells (CD4⁺) coordinate the immune response but do not directly kill infected cells.
Section B: Structured Questions [30 marks]
11. (a) 2 marks
Answer: The AV valve closes at approximately 0.1 s (or at point X, where ventricular pressure exceeds atrial pressure).
Explanation: The AV valve closes when the pressure in the left ventricle exceeds the pressure in the left aorta/left ventricle during the onset of ventricular systole. On the graph, this corresponds to the point where the ventricular pressure curve begins to rise sharply above the atrial pressure curve (point X). At this moment, the backflow of blood pushes the AV valve shut, preventing regurgitation into the atrium.
Marking: 1 mark for correct time/point identification + 1 mark for explanation linking pressure change to valve closure.
11. (b) 3 marks
Answer: Between points X and Y, the left ventricle undergoes isovolumetric contraction. Both the AV valve and the semilunar (aortic) valve are closed. The ventricular muscle contracts, causing a rapid increase in pressure without any change in volume (no blood is ejected yet). The pressure rises from approximately 0 mmHg to ~80 mmHg (the aortic diastolic pressure threshold), at which point the semilunar valve opens.
Marking:
- 1 mark: Isovolumetric contraction identified.
- 1 mark: Both valves closed, volume constant.
- 1 mark: Pressure rises sharply due to ventricular muscle contraction; semilunar valve opens when ventricular pressure exceeds aortic pressure.
11. (c) 3 marks
Answer: Between points Y and Z, the ventricular ejection phase occurs. The semilunar (aortic) valve is open, and blood is ejected from the left ventricle into the aorta. Ventricular pressure rises to a peak (~120 mmHg at point Y) and then begins to fall as blood leaves the ventricle. Ventricular volume decreases rapidly as blood is expelled. At point Z, ventricular pressure falls below aortic pressure, causing backflow of blood that closes the semilunar valve.
Marking:
- 1 mark: Ventricular ejection identified.
- 1 mark: Blood ejected into aorta; volume decreases.
- 1 mark: Semilunar valve closes at Z when ventricular pressure drops below aortic pressure.
12. (a) 4 marks
Answer:
- The action potential arrives at the axon terminal (presynaptic membrane) of the motor neurone, causing depolarisation.
- Voltage-gated calcium channels open, and Ca²⁺ ions flow into the axon terminal down their concentration gradient.
- The influx of Ca²⁺ causes synaptic vesicles containing acetylcholine (ACh) to fuse with the presynaptic membrane and release ACh into the synaptic cleft by exocytosis.
- ACh diffuses across the synaptic cleft and binds to specific ligand-gated sodium channels (nicotinic receptors) on the motor end plate of the muscle fibre.
- The binding of ACh opens the ligand-gated channels, allowing Na⁺ to enter the muscle fibre, causing depolarisation of the motor end plate (end-plate potential).
- If the end-plate potential reaches threshold, an action potential is generated in the muscle fibre membrane (sarcolemma).
Marking: 1 mark each for any 4 of the above points. Must include: Ca²⁺ entry, ACh release by exocytosis, binding to receptors on motor end plate, depolarisation of muscle fibre.
12. (b) 5 marks
Answer:
- When an action potential arrives at the neuromuscular junction, Ca²⁺ is released from the sarcoplasmic reticulum (SR) into the sarcoplasm of the muscle fibre.
- Ca²⁺ binds to troponin on the thin (actin) filament, causing a conformational change that moves tropomyosin away from the myosin-binding sites on actin.
- The myosin head (in its high-energy conformation, with ADP + Pᵢ attached) binds to the exposed binding site on actin, forming a cross-bridge.
- The power stroke occurs: the myosin head pivots, pulling the actin filament towards the centre of the sarcomere. ADP and Pᵢ are released.
- A new ATP molecule binds to the myosin head, causing it to detach from actin.
- ATP is hydrolysed to ADP + Pᵢ by ATPase on the myosin head, re-cocking the myosin head into its high-energy position.
- The cycle repeats as long as Ca²⁺ and ATP are available, causing the actin filaments to slide past the myosin filaments, shortening the sarcomere (muscle contraction).
Marking:
- 1 mark: Ca²⁺ release from SR and binding to troponin.
- 1 mark: Tropomyosin moves, exposing binding sites on actin.
- 1 mark: Cross-bridge formation and power stroke.
- 1 mark: ATP binding causes detachment; ATP hydrolysis re-cocks myosin head.
- 1 mark: Repeated cycling causes sliding of filaments, sarcomere shortens.
13. (a) 2 marks
Answer: Protein molecules (e.g., albumin, globulins) are too large to pass through the filtration barrier in the glomerulus. The barrier consists of the fenestrated endothelium of the glomerular capillaries, the basement membrane, and the podocytes of the Bowman's capsule. These layers prevent molecules with a molecular weight above approximately 68,000 (such as most plasma proteins) from entering the filtrate.
Marking: 1 mark for stating proteins are too large + 1 mark for reference to the filtration barrier (endothelium, basement membrane, or podocytes).
13. (b) 2 marks
Answer: Glucose is a small molecule that is freely filtered at the glomerulus, so it appears in the glomerular filtrate at the same concentration as in plasma. In the proximal convoluted tubule (PCT), glucose is completely reabsorbed by active transport (co-transport with Na⁺ via SGLT transporters on the apical membrane) and facilitated diffusion (GLUT transporters on the basal membrane) into the blood. Therefore, no glucose appears in the urine of a healthy person.
Marking: 1 mark for glucose being freely filtered + 1 mark for complete reabsorption in PCT by active transport/co-transport.
13. (c) 2 marks
Answer: Urea is a small nitrogenous waste product that is freely filtered at the glomerulus. As the filtrate passes along the nephron, a large proportion of water is reabsorbed (approximately 99% of filtered water), particularly in the PCT and the Loop of Henle. Since urea is not significantly reabsorbed (and some is passively reabsorbed in the collecting duct), it becomes concentrated in the remaining fluid. The removal of water without proportional removal of urea results in a much higher concentration of urea in the urine compared to plasma.
Marking: 1 mark for urea being freely filtered + 1 mark for water reabsorption concentrating urea in the remaining filtrate.
13. (d) 2 marks
Answer: Although sodium ions are actively reabsorbed in the PCT (approximately 65%), Loop of Henle, and distal tubule, the reabsorption of water along the nephron (especially in the Loop of Henle and collecting duct under ADH control) is proportionally greater. This means that while the total amount of Na⁺ in the urine is less than what was filtered, the concentration of Na⁺ in the urine is higher because the urine volume is much smaller than the original filtrate volume. Additionally, aldosterone promotes Na⁺ reabsorption in the distal tubule and collecting duct, but the final urine still has a higher concentration due to water conservation.
Marking: 1 mark for water reabsorption being proportionally greater than Na⁺ reabsorption + 1 mark for resulting concentration effect (smaller urine volume).
14. (a) 3 marks)
Answer:
| Feature | Innate Immunity | Adaptive Immunity |
|---|---|---|
| Specificity | Non-specific; responds to general pathogen-associated molecular patterns (PAMPs) | Specific; recognises specific antigens via receptors on B and T cells |
| Response time | Immediate (minutes to hours) | Slower (days to weeks for primary response) |
| Memory | No immunological memory; same response on re-exposure | Has immunological memory; faster and stronger secondary response |
| Key components | Physical barriers (skin, mucous membranes), phagocytes (neutrophils, macrophages), complement proteins, natural killer cells, inflammation | B lymphocytes (produce antibodies), T lymphocytes (helper and cytotoxic), antigen-presenting cells |
Marking: 1 mark each for any 3 valid distinguishing points (specificity, response time, or memory must be included for full marks).
14. (b) 4 marks
Answer:
- When a pathogen enters the body, antigens from the pathogen are processed and presented on the surface of antigen-presenting cells (APCs), such as dendritic cells and macrophages, in association with MHC class II molecules.
- Clonal selection: Among the vast population of naïve B lymphocytes, only those whose surface immunoglobulin (B cell receptor) specifically binds to the antigen are selected. This is clonal selection — the antigen selects the specific B cell clone.
- The selected B cell is activated (with help from helper T cells, which release cytokines such as interleukin-2).
- Clonal expansion: The activated B cell undergoes repeated mitotic divisions, producing a large population of identical clones.
- These clones differentiate into plasma cells (which secrete large quantities of specific antibodies) and memory B cells (which persist in the body and provide long-term immunological memory for a faster secondary response).
Marking:
- 1 mark: Antigen presentation by APC / antigen binding to specific B cell receptor.
- 1 mark: Clonal selection — only B cells with complementary receptor are activated.
- 1 mark: Clonal expansion — mitotic division producing many identical clones.
- 1 mark: Differentiation into plasma cells (secrete antibodies) and memory B cells.
15. (a) 2 marks
Answer: Two ways insulin lowers blood glucose:
- Insulin stimulates glycogenesis — the conversion of glucose to glycogen in liver and muscle cells.
- Insulin increases the uptake of glucose by target cells (especially muscle and adipose tissue) by promoting the translocation of GLUT4 transporters to the cell membrane.
(Also acceptable: insulin promotes conversion of glucose to fat in adipose tissue; insulin inhibits glycogenolysis and gluconeogenesis in the liver.)
Marking: 1 mark each for any 2 valid ways.
15. (b) 2 marks
Answer: Blood glucose regulation is a negative feedback mechanism because the response (change in hormone secretion) counteracts the original stimulus, returning the blood glucose level to its set point (approximately 5 mmol/L or 90 mg/100 mL). When blood glucose rises above normal, insulin is secreted, which lowers blood glucose. When blood glucose falls below normal, glucagon is secreted, which raises blood glucose. In each case, the effect opposes the deviation from the set point, which is the defining feature of negative feedback.
Marking: 1 mark for stating that the response counteracts/reverses the stimulus + 1 mark for linking to the specific example (insulin/glucagon opposing the change in blood glucose).
15. (c) 3 marks
Answer: In Type II diabetes, target cells (especially liver, muscle, and adipose tissue) become resistant to the action of insulin. This means that even though insulin is produced and secreted by beta cells, the target cells do not respond effectively — GLUT4 transporters are not adequately translocated to the cell membrane, glycogenesis is reduced, and glucose uptake is impaired. As a result, blood glucose remains elevated after a meal. The pancreas initially compensates by producing more insulin (hyperinsulinaemia), but over time beta cell function may decline. The persistently elevated blood glucose is due to the failure of insulin signalling at the target cell level.
Marking:
- 1 mark: Target cells do not respond to insulin (insulin resistance).
- 1 mark: Reduced glucose uptake / reduced glycogenesis / GLUT4 not translocated.
- 1 mark: Blood glucose remains elevated because the normal response to insulin is impaired.
16. (a) 4 marks
Answer:
- The hypothalamus acts as the body's thermostat, containing thermoreceptors that monitor the temperature of the blood flowing through it (core body temperature).
- The hypothalamus also receives input from peripheral thermoreceptors in the skin, providing information about external temperature.
- If core temperature deviates from the set point (~37 °C), the hypothalamus coordinates appropriate effector responses via the autonomic nervous system and endocrine signals.
- If temperature is too high, the hypothalamus triggers vasodilation of skin blood vessels, sweating, and behavioural responses (e.g., seeking shade).
- If temperature is too low, the hypothalamus triggers vasoconstriction of skin blood vessels, shivering, increased metabolic rate, and behavioural responses (e.g., putting on clothing).
- The hypothalamus also stimulates the release of thyroid hormones (via TRH → TSH) to increase basal metabolic rate for long-term thermoregulation.
Marking:
- 1 mark: Hypothalamus contains thermoreceptors monitoring core blood temperature.
- 1 mark: Receives input from peripheral thermoreceptors.
- 1 mark: Coordinates responses via autonomic nervous system.
- 1 mark: Triggers appropriate heat-loss or heat-gain mechanisms.
16. (b) 4 marks
Answer:
- Vasoconstriction: The hypothalamus stimulates sympathetic nerves causing constriction of arterioles in the skin. This reduces blood flow to the skin surface, reducing heat loss by radiation, convection, and conduction.
- Shivering: The hypothalamus activates skeletal muscles to undergo rapid, involuntary contractions (shivering). This increases metabolic activity in muscles, generating heat as a byproduct of increased cellular respiration (ATP hydrolysis).
- Metabolic response: The hypothalamus stimulates the release of adrenaline from the adrenal medulla and thyroid hormones (via the hypothalamic-pituitary-thyroid axis). Adrenaline increases metabolic rate in many tissues. Thyroid hormones (T3 and T4) increase basal metabolic rate over a longer period, increasing heat production.
- Piloerection: Arrector pili muscles contract, causing hairs to stand erect. In humans, this has minimal thermoregulatory effect but is a vestigial response.
- Reduced sweating: Eccrine sweat glands reduce or cease secretion, minimising evaporative heat loss.
Marking:
- 1 mark: Vasoconstriction reduces blood flow to skin, reducing heat loss.
- 1 mark: Shivering increases heat production via muscle contraction/metabolism.
- 1 mark: Adrenaline and thyroid hormones increase metabolic rate/heat production.
- 1 mark: Reduced sweating / piloerection (any valid additional point).
Section C: Free Response Questions [20 marks]
17. [8 marks]
Answer:
- At rest, the neurone has a resting membrane potential of approximately −70 mV, maintained by the sodium-potassium pump and K⁺ leak channels.
- When a stimulus is received, voltage-gated sodium channels open, and Na⁺ rushes into the neurone, causing depolarisation. If threshold is reached, an action potential is generated (all-or-nothing principle).
- The action potential at one point on the axon causes local currents that depolarise the adjacent region to threshold, propagating the impulse along the axon.
- In a myelinated neurone, the myelin sheath (formed by Schwann cells in the PNS) acts as an electrical insulator, preventing ion exchange across the membrane at the myelinated regions.
- Action potentials can only occur at the Nodes of Ranvier, where the myelin sheath is absent and voltage-gated ion channels are concentrated. The action potential "jumps" from node to node — this is called saltatory conduction.
- Saltatory conduction significantly increases the speed of nerve impulse transmission because depolarisation only occurs at discrete points, and the electrical signal is conducted rapidly through the myelinated internodal segments by local currents.
- After depolarisation, voltage-gated sodium channels enter an inactivated state (refractory period), and voltage-gated potassium channels open, allowing K⁺ to leave the cell, causing repolarisation.
- The sodium-potassium pump restores the resting ion distribution.
Marking:
- 1 mark: Resting potential and depolarisation by Na⁺ influx.
- 1 mark: Threshold and all-or-nothing principle.
- 1 mark: Local currents propagate the action potential.
- 1 mark: Myelin sheath as insulator.
- 1 mark: Action potential only at Nodes of Ranvier.
- 1 mark: Saltatory conduction and increased speed.
- 1 mark: Repolarisation by K⁺ efflux.
- 1 mark: Refractory period / sodium-potassium pump restores resting state.
18. [7 marks]
Answer:
- Carbonic acid–hydrogen carbonate buffer system: This is the most important buffer in blood plasma. The equilibrium is: CO₂ + H₂O ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻. When H⁺ concentration increases (pH falls), the equilibrium shifts to the left, removing excess H⁺. When H⁺ concentration decreases (pH rises), the equilibrium shifts to the right, releasing H⁺. This system maintains pH within the narrow range of 7.35–7.45.
- Respiratory system: If blood pH falls (more acidic), chemoreceptors in the medulla oblongata and aortic/carotid bodies detect the increase in H⁺ / CO₂. The respiratory centre increases the rate and depth of breathing, expelling more CO₂. This shifts the buffer equilibrium to the left, reducing H⁺ concentration and raising pH back to normal. Conversely, if blood pH rises, breathing rate decreases, retaining CO₂ and lowering pH.
- Kidneys: The kidneys regulate blood pH by controlling the excretion of H⁺ and HCO₃⁻. In the PCT and distal tubule, H⁺ ions are actively secreted into the tubular fluid, where they are buffered by phosphate ions (HPO₄²⁻ → H₂PO₄⁻) or ammonia (NH₃ + H⁺ → NH₄⁺) and excreted in urine. Simultaneously, HCO₃⁻ is reabsorbed into the blood. If blood is too alkaline, less H⁺ is secreted and more HCO₃⁻ is excreted. The kidneys provide long-term pH regulation (hours to days), complementing the rapid respiratory response.
Marking:
- 2 marks: Buffer system equilibrium and how it resists pH change (both directions).
- 2 marks: Respiratory response — chemoreceptors detect CO₂/H⁺, increased ventilation removes CO₂, shifts equilibrium.
- 2 marks: Kidneys secrete H⁺, reabsorb HCO₃⁻, use buffers in urine (phosphate/ammonia), long-term regulation.
- 1 mark: Integration — all three systems work together to maintain pH 7.35–7.45.
19. [5 marks]
Answer:
| Feature | Humoral Immune Response | Cell-Mediated Immune Response |
|---|---|---|
| Key cells | B lymphocytes | Cytotoxic T cells (CD8⁺) |
| Target | Extracellular pathogens (bacteria, viruses in blood/lymph, toxins) | Intracellular pathogens (virus-infected cells, cancer cells, transplanted cells) |
| Mechanism | B cells differentiate into plasma cells that secrete antibodies. Antibodies bind to specific antigens, neutralising pathogens, promoting opsonisation, and activating complement. | Cytotoxic T cells recognise antigens on MHC class I of infected cells. They release perforin (forms pores) and granzymes (trigger apoptosis), directly killing the target cell. |
| Antigen presentation | Antigens recognised directly by B cell receptor (surface immunoglobulin) | Antigens must be presented on MHC class I molecules (all nucleated cells) |
| Memory | Memory B cells provide long-term humoral immunity | Memory T cells provide long-term cell-mediated immunity |
Similarities: Both are specific adaptive immune responses; both involve clonal selection and clonal expansion; both generate memory cells for long-term immunity; both require activation by helper T cells (CD4⁺) in most cases.
Marking:
- 1 mark: B cells vs. cytotoxic T cells.
- 1 mark: Extracellular vs. intracellular targets.
- 1 mark: Antibodies (humoral) vs. direct cell killing via perforin/granzymes (cell-mediated).
- 1 mark: Antigen recognition differences (free antigen vs. MHC I presentation).
- 1 mark: Valid similarity stated.
20. (a) 2 marks
Answer:
Cardiac output = Heart rate × Stroke volume
During exercise: Heart rate = 155 beats/min; Tidal volume is given but stroke volume is not directly stated. However, the question asks for cardiac output and provides heart rate and tidal volume. Since stroke volume is not given, we assume the question intends for the student to use the tidal volume as a proxy or the question expects recognition that stroke volume data is needed.
Re-reading the question: The table provides heart rate, breathing rate, and tidal volume. Cardiac output requires stroke volume, which is not provided. However, a typical A-Level question would provide stroke volume. Given the data, the most reasonable interpretation is that the question expects the student to calculate cardiac output using heart rate and an implied stroke volume. Since stroke volume is not given, the question may contain an oversight. For the purposes of this answer, we will assume a typical exercise stroke volume of ~110 mL (a reasonable estimate for a healthy student during moderate exercise).
Revised interpretation: The question likely intends for students to recognise that cardiac output = heart rate × stroke volume, and that stroke volume can be estimated or is implied. However, since the table does not provide stroke volume, the question as written is incomplete.
For marking purposes, assuming stroke volume during exercise = 110 mL:
Cardiac output = 155 beats/min × 110 mL/beat = 17,050 mL/min = 17.05 L/min
Marking:
- 1 mark for correct formula (CO = HR × SV).
- 1 mark for correct calculation and unit (L/min).
Note to examiner: The question should provide stroke volume data. If not provided, accept any reasonable calculation based on stated assumptions.
20. (b) 4 marks
Answer:
- During exercise, skeletal muscles require more ATP for contraction, increasing the rate of cellular respiration. This produces more CO₂, which dissolves in blood to form carbonic acid, lowering blood pH.
- Chemoreceptors in the medulla oblongata and aortic/carotid bodies detect the rise in CO₂ / H⁺ (fall in pH).
- These chemoreceptors send impulses to the cardiac centre in the medulla oblongata, which increases heart rate via sympathetic nerve stimulation (and decreased parasympathetic/vagal tone). This increases cardiac output, delivering more oxygen and glucose to the muscles and removing CO₂ faster.
- Simultaneously, the respiratory centre in the medulla increases the rate and depth of breathing (increased breathing rate and tidal volume), enhancing gas exchange in the alveoli — more O₂ is taken in and more CO₂ is expelled.
- Additionally, proprioceptors in muscles and joints detect movement and send impulses to the respiratory and cardiac centres, contributing to the anticipatory increase in heart rate and breathing rate at the onset of exercise.
Marking:
- 1 mark: Increased CO₂ from respiration lowers blood pH.
- 1 mark: Chemoreceptors detect pH/CO₂ changes.
- 1 mark: Cardiac centre increases heart rate (sympathetic stimulation).
- 1 mark: Respiratory centre increases breathing rate and depth; proprioceptors contribute.
20. (c) 3 marks
Answer:
- During exercise, lactic acid accumulates in muscles due to anaerobic respiration when oxygen supply is insufficient. After exercise stops, the lactic acid must be removed — it is transported to the liver where it is converted back to glucose (Cori cycle) or oxidised to CO₂ and H₂O. This process requires additional oxygen (oxygen debt).
- The elevated heart rate and breathing rate continue post-exercise to supply the extra oxygen needed to repay the oxygen debt, metabolise accumulated lactic acid, resynthesise creatine phosphate stores, and restore oxygen levels in myoglobin and haemoglobin.
- Body temperature remains elevated after exercise, and the metabolic rate is still high. The heart rate and breathing rate remain elevated to support the increased metabolic demands and to dissipate excess heat through increased blood flow to the skin and continued ventilation.
Marking:
- 1 mark: Oxygen debt / lactic acid removal requires continued elevated oxygen supply.
- 1 mark: Resynthesis of creatine phosphate, restoration of O₂ stores.
- 1 mark: Elevated metabolic rate / body temperature requires continued elevated cardiac and respiratory function.
Free quiz and exam paper access
Enter your details to view this paper
Your access is remembered on this device.