From Real Exams Quiz
A Level H1 Biology Human Physiology Quiz
Free A Level H1 Biology Human Physiology quiz, LongCat Exam version, with questions, answers, and A Level-style practice for Singapore students.
These static practice materials are generated from the site's syllabus and paper-generation workflow, with source and model context shown so students and parents can evaluate the material before use.
Questions
A-Level Biology H1 Quiz - Human Physiology
Name: ___________________________
Class: ___________________________
Date: ___________________________
Score: ________ / 50
Duration: 60 minutes
Total Marks: 50
Instructions:
- Answer ALL questions.
- Write your answers in the spaces provided.
- The number of marks for each question is shown in brackets [ ].
- Where a question requires explanation or reasoning, answers must be written in clear, concise biological language.
- The total marks for this paper is 50.
Section A: Short Answer Questions (Questions 1–10)
Answer ALL questions. Each question carries 2 marks unless otherwise stated.
1. State two functions of the lymphatic system in human physiology.
[2]
2. Distinguish between innate immunity and adaptive immunity by stating one key feature of each.
Innate immunity: _____________________________________________________________
Adaptive immunity: ___________________________________________________________
[2]
3. Fig. 3.1 shows a schematic diagram of an antibody molecule.
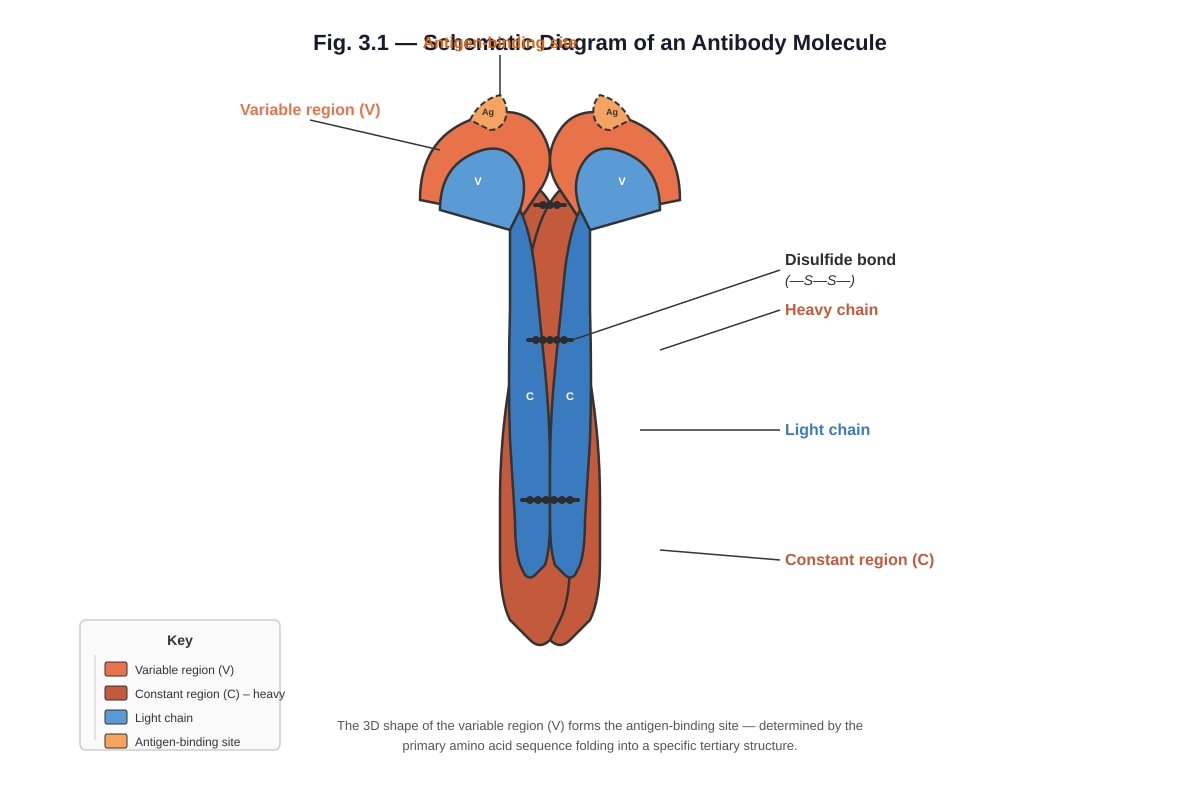
Generated diagram for Q3.
With reference to Fig. 3.1, state the level of protein structure that determines the shape of the antigen-binding site.
[2]
4. Explain why antibodies produced during a secondary immune response are more effective than those produced during a primary immune response.
[2]
5. State two ways in which a retrovirus such as HIV differs from a typical DNA virus in its replication cycle.
(i) _________________________________________________________________________
(ii) ________________________________________________________________________
[2]
6. Define the term antigen in the context of the immune response.
[2]
7. Explain why vaccination provides long-term protection against a specific pathogen.
[2]
8. State two physical barriers that form part of the body's first line of defence against pathogens.
(i) _________________________________________________________________________
(ii) ________________________________________________________________________
[2]
9. Describe the role of helper T-lymphocytes in the adaptive immune response.
[2]
10. Explain the term herd immunity and state one condition required for it to be effective.
Herd immunity: _____________________________________________________________
Condition: _________________________________________________________________
[2]
Section B: Structured Response (Questions 11–17)
Answer ALL questions.
11. Fig. 11.1 shows the concentration of antibody in the blood of an individual following two separate injections of the same antigen, given at Day 0 and Day 28.
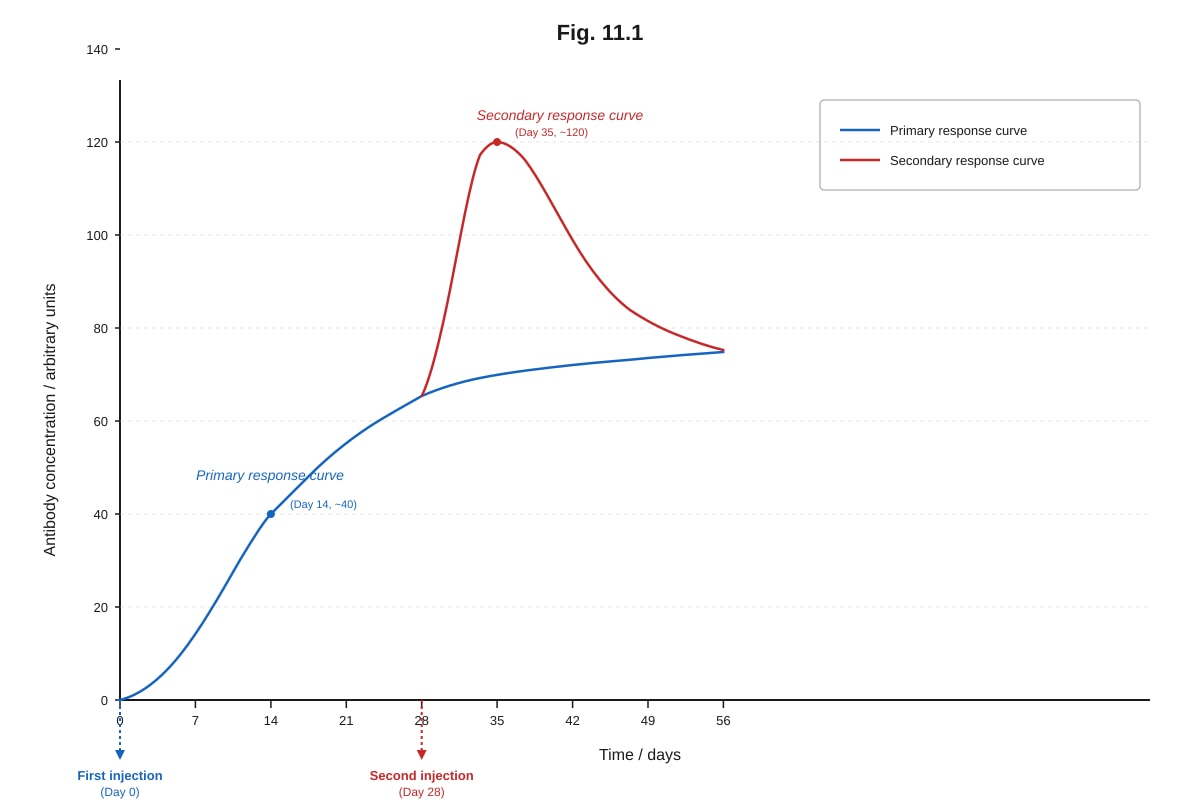
Generated graph for Q11.
(a) With reference to Fig. 11.1, describe the differences between the primary and secondary immune responses.
[2]
(b) Explain the immunological basis for the difference in antibody concentration between the primary and secondary responses.
[3]
[Total: 5]
12. Fig. 12.1 shows the process of phagocytosis.
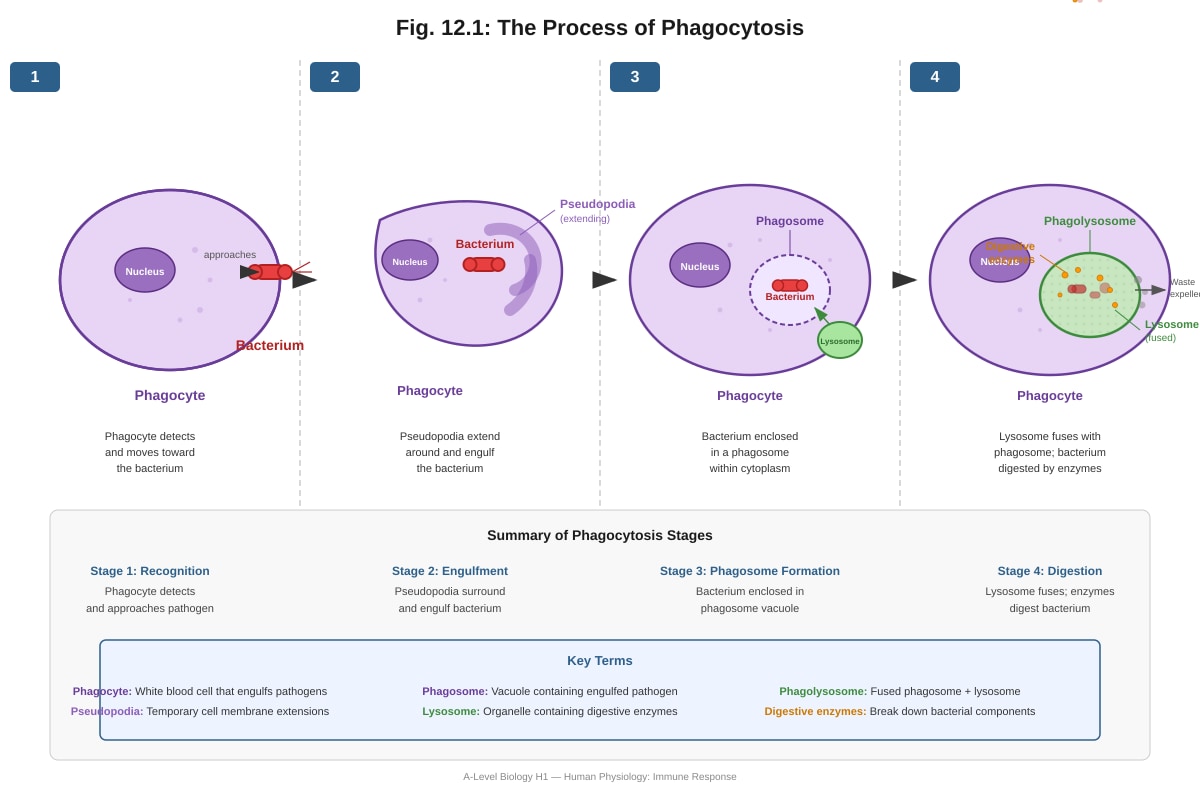
Generated diagram for Q12.
(a) With reference to Fig. 12.1, describe how the bacterium is destroyed after it has been engulfed by the phagocyte.
[2]
(b) Explain how the products of digestion are then processed and presented by the phagocyte to other immune cells.
[2]
[Total: 4]
13. Tuberculosis (TB) is caused by the bacterium Mycobacterium tuberculosis. The World Health Organization recommends the BCG vaccine for infants in countries where TB is common.
(a) Explain how the BCG vaccine stimulates immunity against tuberculosis.
[3]
(b) Despite widespread vaccination, TB remains a major global health problem. Suggest two reasons why vaccination alone has not eliminated TB.
(i) _________________________________________________________________________
(ii) ________________________________________________________________________
[2]
[Total: 5]
14. Fig. 14.1 shows a simplified diagram of the human breathing system.
Image pending generation: diagram for Q14.
(a) With reference to Fig. 14.1, state two structural features of alveoli that make them efficient surfaces for gas exchange.
(i) _________________________________________________________________________
(ii) ________________________________________________________________________
[2]
(b) Explain how the breathing mechanism (inspiration) brings air into the lungs.
[2]
[Total: 4]
15. Fig. 15.1 shows a section through the human heart as seen from the front.
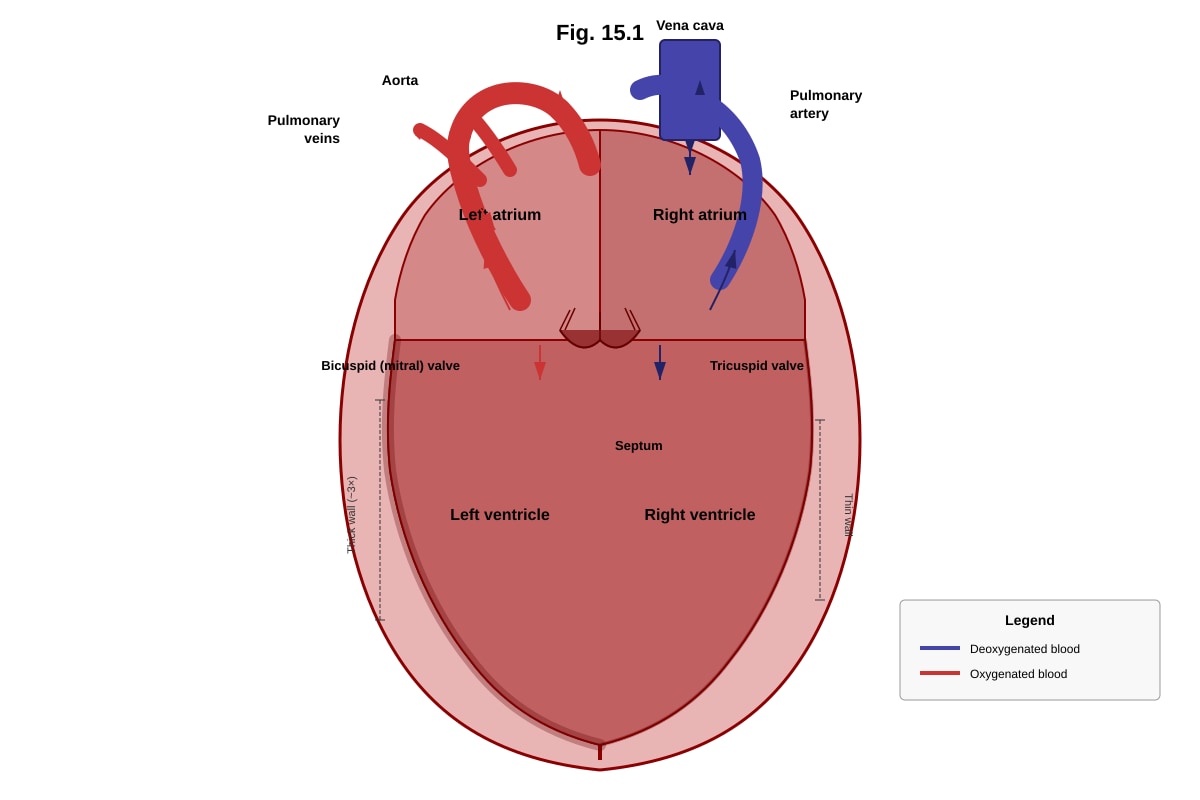
Generated diagram for Q15.
(a) With reference to Fig. 15.1, state which blood vessel carries oxygenated blood away from the heart.
[1]
(b) Explain why the wall of the left ventricle is thicker than the wall of the right ventricle.
[2]
(c) Describe the role of the valves in the heart during one complete heartbeat.
[2]
[Total: 5]
16. Fig. 16.1 shows the changes in pressure and volume in the left side of the heart and the aorta during one cardiac cycle.
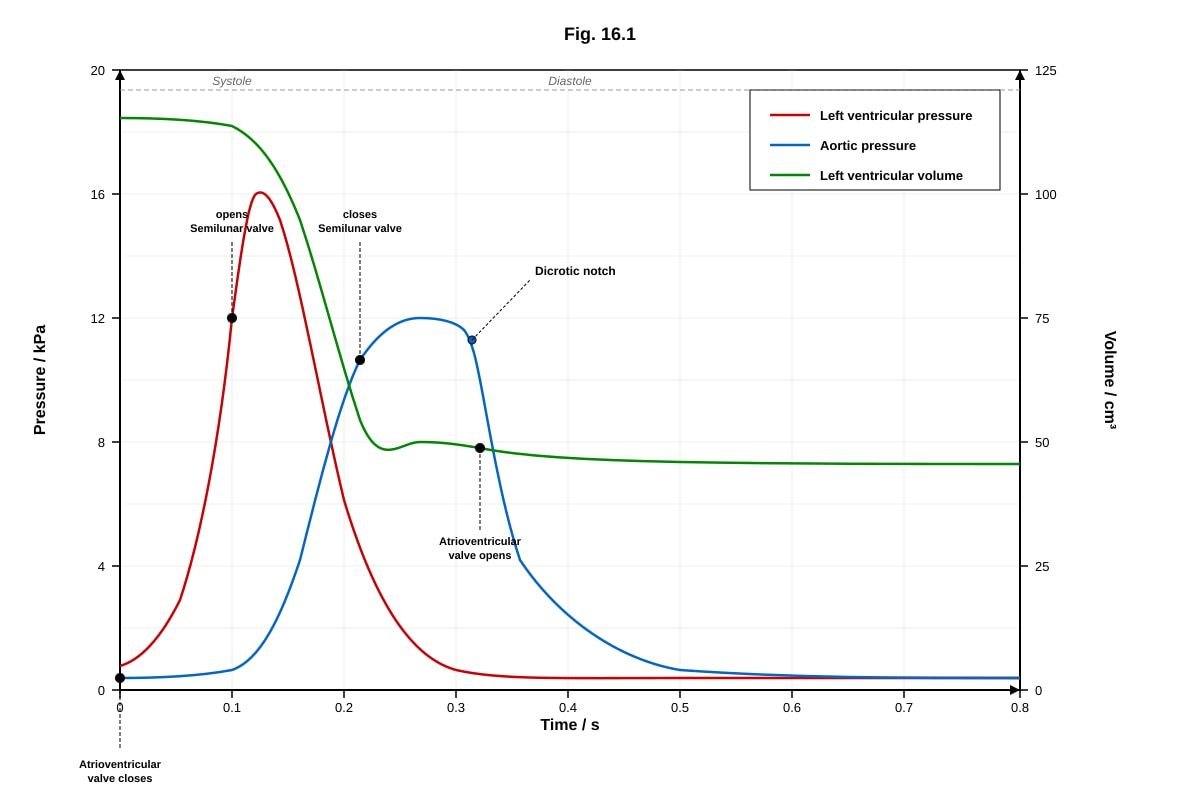
Generated graph for Q16.
(a) With reference to Fig. 16.1, state the time at which the semilunar valve opens.
[1]
(b) Explain the cause of the dicrotic notch seen in the aortic pressure curve.
[2]
(c) Calculate the heart rate in beats per minute based on the information in Fig. 16.1. Show your working.
[2]
[Total: 5]
17. A student carried out an experiment to investigate the effect of exercise on heart rate. The resting heart rate of the student was measured, and then the student exercised for 5 minutes. The heart rate was measured immediately after exercise and at 2-minute intervals during recovery. The results are shown in Table 17.1.
Table 17.1
| Time after exercise / min | Heart rate / beats per min |
|---|---|
| 0 (resting) | 72 |
| 0 (immediately after) | 156 |
| 2 | 120 |
| 4 | 96 |
| 6 | 84 |
| 8 | 76 |
| 10 | 72 |
(a) Calculate the percentage increase in heart rate from resting to immediately after exercise. Show your working.
[2]
(b) Explain why the heart rate increases during exercise.
[2]
(c) Suggest why the heart rate does not return to resting level immediately after exercise stops.
[2]
[Total: 6]
Section C: Data-Based and Extended Response (Questions 18–20)
Answer ALL questions.
18. Read the following passage and answer the questions below.
Influenza is a contagious respiratory illness caused by influenza viruses. The virus infects the epithelial cells of the respiratory tract, leading to symptoms such as fever, cough, and body aches. Antigenic drift involves small, gradual mutations in the genes coding for the viral surface proteins haemagglutinin (H) and neuraminidase (N). These mutations alter the shape of the surface proteins so that antibodies from a previous infection or vaccination may no longer bind effectively. Antigenic shift, on the other hand, occurs when two different influenza viruses infect the same cell and exchange entire gene segments, producing a novel subtype against which the human population has little or no pre-existing immunity. This can lead to pandemics.
(a) Explain why antigenic drift can reduce the effectiveness of a flu vaccine from a previous year.
[2]
(b) Distinguish between antigenic drift and antigenic shift.
[2]
(c) Explain why antigenic shift poses a greater public health threat than antigenic drift.
[2]
[Total: 6]
19. Fig. 19.1 shows the effect of different concentrations of a bacterial toxin on the growth of a human cell culture over 48 hours.
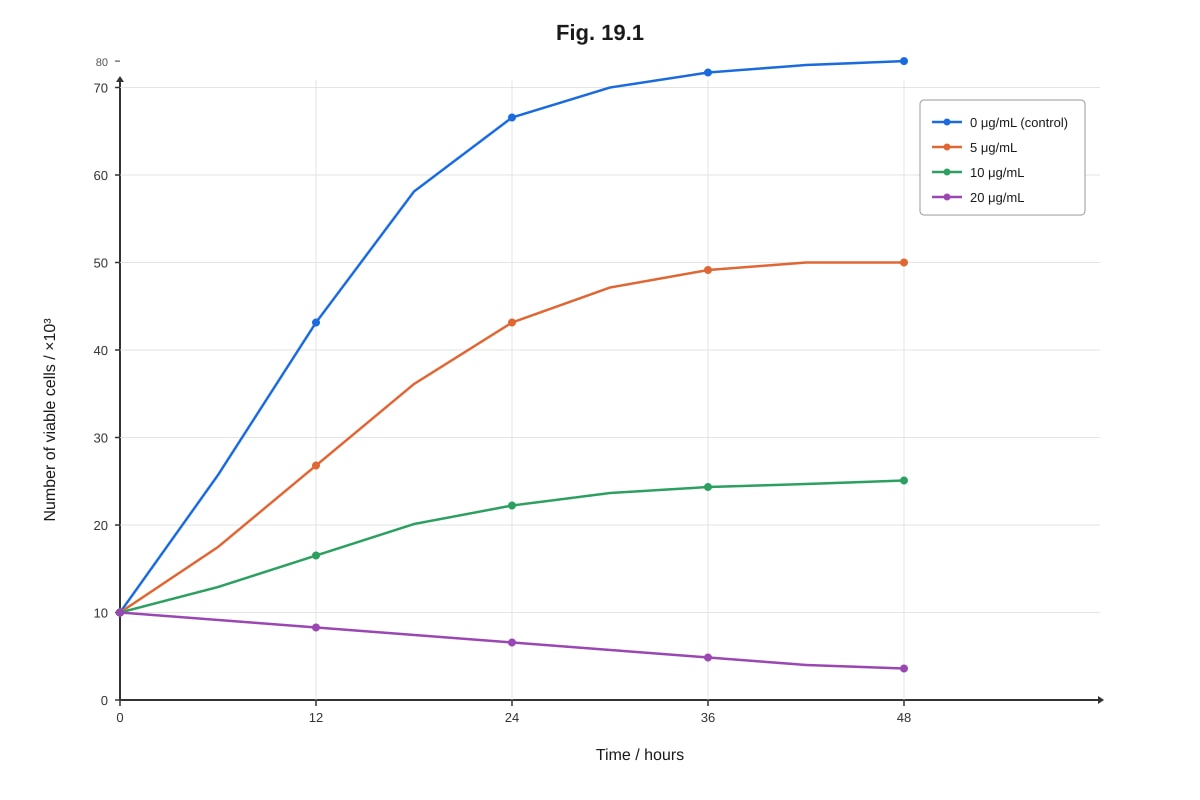
Generated graph for Q19.
(a) With reference to Fig. 19.1, describe the effect of increasing toxin concentration on cell growth.
[2]
(b) Suggest a mechanism by which the bacterial toxin could be causing the observed effects on the human cells.
[2]
(c) Explain how the innate immune system would respond to an infection by this bacterium in the body.
[3]
[Total: 7]
20. Discuss the role of both the specific and non-specific immune responses in protecting the human body against infectious disease. In your answer, include named examples of cells, molecules, and processes involved.
[8]
END OF PAPER
Total Marks: 50
Answers
A-Level Biology H1 Quiz - Human Physiology
Answer Key
Section A: Short Answer Questions (Questions 1–10)
1. [2 marks]
Two functions of the lymphatic system:
- Return of excess tissue fluid (interstitial fluid) to the bloodstream – The lymphatic system collects fluid that leaks from blood capillaries into tissue spaces and returns it to the venous circulation via the thoracic duct and right lymphatic duct, preventing oedema.
- Transport of fats from the small intestine – Lacteals (lymphatic capillaries in intestinal villi) absorb fatty acids and glycerol packaged into chylomicrons, transporting them as lymph.
- (Also acceptable: Transport of lymphocytes and immune surveillance; filtration of lymph through lymph nodes where pathogens are trapped and destroyed by lymphocytes and macrophages.)
Marking: 1 mark per correct function, any 2.
2. [2 marks]
- Innate immunity: Provides a rapid, non-specific response – it does not distinguish between different types of pathogens and responds to all in the same general way. (Also acceptable: present from birth; does not involve memory cells; includes physical barriers, phagocytes, inflammation.)
- Adaptive immunity: Provides a specific response targeted to a particular antigen/pathogen and generates immunological memory, so that a second exposure produces a faster, stronger response. (Also acceptable: involves B and T lymphocytes; takes days to develop on first exposure; produces memory cells.)
Marking: 1 mark for each correct distinguishing feature.
3. [2 marks]
The shape of the antigen-binding site is determined by the tertiary structure of the protein.
Explanation: The antibody is a protein made of polypeptide chains. The tertiary structure refers to the three-dimensional folding of each polypeptide chain, which creates the specific shape of the variable region at the tips of the Y. It is this 3D conformation that determines the precise shape of the antigen-binding site, allowing it to bind specifically to a complementary antigen. The amino acid sequence (primary structure) determines how the protein folds, but it is the final 3D folded shape — the tertiary structure — that directly creates the binding site geometry.
Common mistake: Students may answer "primary structure." While the amino acid sequence ultimately determines the shape, the question asks which level of structure determines the shape of the binding site — this is the tertiary (3D folded) structure.
Marking: 1 mark for "tertiary structure"; 1 mark for explanation linking 3D folding to the specific shape of the antigen-binding site.
4. [2 marks]
During the primary immune response, antigen-specific B-lymphocytes are activated, proliferate (clonal expansion), and differentiate into plasma cells (which secrete antibodies) and memory B-cells. This process takes several days. Upon second exposure to the same antigen, memory B-cells are already present in large numbers. They are activated much more rapidly, undergo faster clonal expansion, and differentiate into plasma cells that produce greater quantities of antibody in a shorter time. The antibodies produced also tend to have higher affinity for the antigen due to affinity maturation (somatic hypermutation and selection during the primary response).
Marking: 1 mark for reference to memory cells; 1 mark for explaining faster/greater antibody production (or higher affinity).
5. [2 marks]
Two ways a retrovirus (e.g., HIV) differs from a typical DNA virus:
(i) Retroviruses carry RNA as their genetic material (instead of DNA), and must first convert their RNA into DNA using the enzyme reverse transcriptase before they can integrate into the host genome.
(ii) Retroviruses integrate their DNA copy (provirus) into the host cell's chromosome using the enzyme integrase, becoming a permanent part of the host genome, whereas most DNA viruses do not integrate (or do so rarely).
(Also acceptable: Retroviruses have an envelope derived from the host cell membrane; retroviruses require reverse transcriptase, which DNA viruses do not possess.)
Marking: 1 mark per correct difference, any 2.
6. [2 marks]
An antigen is a molecule (usually a protein or polysaccharide) found on the surface of a pathogen or foreign substance that is recognised as non-self by the immune system and stimulates an immune response, specifically the production of antibodies and/or activation of lymphocytes.
Marking: 1 mark for identifying it as a molecule/protein/polysaccharide on a pathogen; 1 mark for stating it triggers an immune response / is recognised as foreign.
7. [2 marks]
Vaccination introduces an antigen (in the form of an attenuated pathogen, killed pathogen, or subunit) into the body. This stimulates a primary immune response, during which memory B-cells and memory T-cells are generated. These memory cells persist in the body for years or even a lifetime. When the actual pathogen is encountered later, the memory cells are rapidly activated, producing a secondary immune response that is faster and stronger, producing high levels of specific antibodies before the pathogen can establish an infection.
Marking: 1 mark for reference to memory cells being produced; 1 mark for explaining that memory cells enable a rapid secondary response upon re-exposure.
8. [2 marks]
Two physical barriers:
(i) Skin – the outer keratinised layer of dead epithelial cells provides a tough, waterproof physical barrier that prevents pathogen entry.
(ii) Mucous membranes – mucus lining the respiratory, digestive, and urogenital tracts traps pathogens and prevents them from reaching epithelial cells.
(Also acceptable: Cilia in the respiratory tract that sweep mucus and trapped pathogens away; stomach acid (chemical barrier); tears/saliva containing lysozyme.)
Marking: 1 mark per correct barrier, any 2.
9. [2 marks]
Helper T-lymphocytes (CD4⁺ T-cells) play a central coordinating role in the adaptive immune response. When a helper T-cell recognises a specific antigen presented on the surface of an antigen-presenting cell (e.g., a macrophage or dendritic cell) via its T-cell receptor, it becomes activated. The activated helper T-cell then secretes cytokines (chemical signalling molecules) that:
- Stimulate the proliferation and differentiation of B-lymphocytes into plasma cells (which produce antibodies) — this is the humoral response.
- Activate cytotoxic T-lymphocytes (CD8⁺ T-cells) to destroy infected cells — this is the cell-mediated response.
- Enhance the activity of macrophages to destroy engulfed pathogens more effectively.
Without helper T-cells, the adaptive immune response is severely compromised (as seen in AIDS, where HIV destroys helper T-cells).
Marking: 1 mark for stating helper T-cells secrete cytokines; 1 mark for describing activation of B-cells and/or cytotoxic T-cells.
10. [2 marks]
Herd immunity occurs when a sufficiently high proportion of a population is immune to an infectious disease (through vaccination or prior infection), making the spread of the disease from person to person unlikely. This indirectly protects individuals who are not immune (e.g., those who cannot be vaccinated due to medical conditions).
Condition: A high percentage of the population must be immune (the exact threshold depends on the disease — for highly contagious diseases like measles, approximately 90–95% of the population must be immune).
Marking: 1 mark for correct definition of herd immunity; 1 mark for stating that a high proportion of the population must be immune.
Section B: Structured Response (Questions 11–17)
11. [5 marks]
(a) [2 marks]
Differences between primary and secondary immune responses:
- The secondary response produces a higher peak concentration of antibody (~120 units) compared to the primary response (~40 units).
- The secondary response rises more rapidly after the second injection, reaching peak antibody levels in approximately 7 days (Day 28 to Day 35), whereas the primary response takes approximately 14 days (Day 0 to Day 14) to reach its peak.
- The secondary response declines more slowly after the peak compared to the primary response.
Marking: 1 mark per correct difference, any 2.
(b) [3 marks]
During the primary immune response, the antigen is encountered for the first time. Naïve B-lymphocytes specific to the antigen must be activated, undergo clonal expansion, and differentiate into plasma cells and memory B-cells. This process takes time (lag phase of ~10–14 days).
During the secondary immune response, memory B-cells generated during the primary response are already present in large numbers. These memory cells have a lower activation threshold than naïve B-cells, so they are activated more quickly. They undergo rapid clonal expansion and differentiate into plasma cells that secrete large amounts of antibody. Additionally, during the primary response, affinity maturation occurs in germinal centres through somatic hypermutation, so the memory B-cells produce antibodies with higher affinity for the antigen. This explains both the faster onset and the greater magnitude of the secondary response.
Marking: 1 mark for reference to memory B-cells; 1 mark for explaining faster activation/lower threshold; 1 mark for explaining greater antibody production (or affinity maturation).
12. [4 marks]
(a) [2 marks]
After the bacterium is engulfed into a phagosome, lysosomes within the phagocyte fuse with the phagosome to form a phagolysosome. The lysosomes contain digestive enzymes (such as lysozyme and hydrolytic enzymes) that break down the bacterium. Reactive oxygen species (e.g., hydrogen peroxide) and other antimicrobial substances within the phagocyte also contribute to destroying the bacterium.
Marking: 1 mark for lysosome fusion forming phagolysosome; 1 mark for digestive enzymes destroying the bacterium.
(b) [2 marks]
After digestion, small peptide fragments (antigens) from the bacterium are loaded onto MHC class II molecules within the phagocyte. These MHC-antigen complexes are transported to the cell surface and presented on the phagocyte's membrane. Helper T-lymphocytes with complementary T-cell receptors recognise the presented antigen and become activated, triggering the adaptive immune response. The phagocyte thus acts as an antigen-presenting cell (APC).
Marking: 1 mark for antigen fragments combined with MHC molecules; 1 mark for presentation to helper T-cells / acting as APC.
13. [5 marks]
(a) [3 marks]
The BCG vaccine contains a live attenuated (weakened) strain of Mycobacterium bovis, which is closely related to M. tuberculosis. When administered, the attenuated bacteria stimulate the immune system as if it were a real infection. Antigen-presenting cells process and present mycobacterial antigens to helper T-lymphocytes, which activate cell-mediated immunity. This leads to the activation and proliferation of specific T-lymphocytes and the generation of memory T-cells. These memory cells persist in the body, so that upon future exposure to M. tuberculosis, a rapid and strong secondary immune response is mounted, preventing the development of active TB.
Marking: 1 mark for reference to attenuated/weakened bacteria acting as antigen; 1 mark for activation of T-cells / cell-mediated immunity; 1 mark for generation of memory cells providing long-term protection.
(b) [2 marks]
Two reasons why vaccination has not eliminated TB:
(i) HIV/AIDS co-infection — HIV destroys helper T-lymphocytes, severely compromising the cell-mediated immunity that is essential for controlling M. tuberculosis. Immunocompromised individuals cannot mount an effective immune response even if previously vaccinated.
(ii) Emergence of drug-resistant strains — Multi-drug resistant (MDR) and extensively drug-resistant (XDR) strains of M. tuberculosis have evolved, making treatment difficult and reducing the effectiveness of public health control measures.
(Also acceptable: BCG vaccine is not 100% effective (variable efficacy 0–80%); incomplete vaccination coverage in developing countries; latent TB infection can reactivate years later; poverty and overcrowding facilitate transmission.)
Marking: 1 mark per valid reason, any 2.
14. [4 marks]
(a) [2 marks]
Two structural features of alveoli for efficient gas exchange:
(i) Very thin walls (one cell thick / squamous epithelium) — the alveolar wall consists of a single layer of flattened epithelial cells, providing a very short diffusion distance for gases.
(ii) Dense network of blood capillaries — each alveolus is surrounded by a rich capillary network, maintaining a steep concentration gradient of oxygen and carbon dioxide between the alveolar air and the blood.
(Also acceptable: Large surface area due to millions of alveoli; moist lining for gases to dissolve before diffusion.)
Marking: 1 mark per correct feature, any 2.
(b) [2 marks]
During inspiration: The external intercostal muscles contract, lifting the rib cage upwards and outwards. Simultaneously, the diaphragm contracts and flattens. These actions increase the volume of the thoracic cavity. According to Boyle's law, an increase in volume causes a decrease in pressure inside the lungs (intrapulmonary pressure drops below atmospheric pressure). Air therefore flows down the pressure gradient from the atmosphere into the lungs.
Marking: 1 mark for describing muscle contraction increasing thoracic volume; 1 mark for linking decreased pressure to air flowing in.
15. [5 marks]
(a) [1 mark]
The aorta carries oxygenated blood away from the heart (from the left ventricle to the rest of the body).
(b) [2 marks]
The left ventricle has a thicker muscular wall because it must generate sufficient pressure to pump blood throughout the entire systemic circulation (to all body tissues), which involves overcoming high resistance over a long distance. The right ventricle only pumps blood to the lungs via the pulmonary circulation, which is a shorter distance with lower resistance, so less pressure is required. The thicker wall of the left ventricle allows it to contract more forcefully.
Marking: 1 mark for stating left ventricle pumps to the whole body (systemic circulation); 1 mark for contrasting with right ventricle pumping only to lungs (shorter distance/lower resistance).
(c) [2 marks]
During atrial systole, the atrioventricular (AV) valves (tricuspid and bicuspid) are open, allowing blood to flow from the atria into the ventricles. When ventricular systole begins, the ventricles contract, causing ventricular pressure to rise sharply. When ventricular pressure exceeds atrial pressure, the AV valves close, producing the first heart sound ("lub") and preventing backflow of blood into the atria. When ventricular pressure exceeds aortic/pulmonary artery pressure, the semilunar valves open, and blood is ejected into the arteries. During diastole, the ventricles relax, and when ventricular pressure falls below arterial pressure, the semilunar valves close, producing the second heart sound ("dub"), preventing backflow into the ventricles.
Marking: 1 mark for describing AV valve closure preventing backflow during ventricular systole; 1 mark for describing semilunar valve closure preventing backflow during diastole.
16. [5 marks]
(a) [1 mark]
The semilunar valve opens at approximately 0.05 s (the point where left ventricular pressure exceeds aortic pressure).
(Accept any value between 0.04–0.06 s depending on reading from the graph.)
(b) [2 marks]
The dicrotic notch is caused by the brief backflow of blood toward the ventricle when ventricular pressure drops below aortic pressure at the end of systole. This backflow causes the semilunar valve to close rapidly, creating a small dip (notch) in the aortic pressure curve. The closure of the semilunar valve prevents blood from flowing back into the left ventricle during diastole.
Marking: 1 mark for backflow of blood when ventricular pressure falls below aortic pressure; 1 mark for closure of the semilunar valve.
(c) [2 marks]
From Fig. 16.1, one complete cardiac cycle takes 0.8 seconds.
Heart rate = 60 seconds ÷ duration of one cycle
Heart rate = 60 ÷ 0.8
Heart rate = 75 beats per minute
Marking: 1 mark for identifying cycle duration as 0.8 s; 1 mark for correct calculation and answer (75 bpm).
17. [6 marks]
(a) [2 marks]
Percentage increase = ((156 − 72) ÷ 72) × 100
= (84 ÷ 72) × 100
= 116.7% (or 117% to 3 s.f.)
Marking: 1 mark for correct working; 1 mark for correct answer.
(b) [2 marks]
During exercise, working muscles require more ATP for contraction, which increases the demand for oxygen and the production of carbon dioxide as a metabolic waste product. Chemoreceptors detect rising CO₂ levels (and falling pH) in the blood and send impulses to the cardiac centre in the medulla oblongata. The cardiac centre increases the frequency of impulses sent via the sympathetic nervous system to the sinoatrial node (SAN), increasing heart rate. This increases cardiac output, delivering more oxygenated blood to the muscles and removing CO₂ more rapidly.
Marking: 1 mark for increased oxygen demand / CO₂ production during exercise; 1 mark for role of chemoreceptors and sympathetic nervous system / cardiac centre increasing heart rate.
(c) [2 marks]
After exercise, the heart rate remains elevated because the body needs to repay the oxygen debt accumulated during exercise. The elevated heart rate continues to supply oxygen to metabolise lactate (produced by anaerobic respiration in muscles during intense exercise) and to restore ATP and creatine phosphate stores. Additionally, the body temperature remains elevated, and CO₂ levels in the blood take time to return to resting levels, so the sympathetic stimulation of the heart continues until homeostasis is restored.
Marking: 1 mark for reference to oxygen debt / lactate removal; 1 mark for continued elevated metabolism / CO₂ clearance / temperature regulation.
Section C: Data-Based and Extended Response (Questions 18–20)
18. [6 marks]
(a) [2 marks]
Antigenic drift involves point mutations in the genes coding for haemagglutinin (H) and neuraminidase (N) surface proteins. These mutations cause small changes in the shape (conformation) of the antigenic sites on these proteins. Antibodies produced from a previous vaccination were shaped to bind to the original antigen shape. Because the antigen shape has changed, the antibodies bind less effectively or fail to recognise the new viral strain, reducing the vaccine's effectiveness.
Marking: 1 mark for mutations altering surface protein shape; 1 mark for reduced antibody binding / recognition.
(b) [2 marks]
- Antigenic drift involves small, gradual mutations in the genes for H and N proteins, resulting in minor changes to surface antigens. This occurs continuously and leads to seasonal flu epidemics.
- Antigenic shift involves the reassortment of entire gene segments between two different influenza viruses co-infecting the same cell, producing a novel subtype (e.g., H1N1 → H5N1) with a dramatically different combination of H and/or N proteins. This occurs rarely but can cause pandemics because the population has little or no pre-existing immunity.
Marking: 1 mark for describing antigenic drift (small mutations, gradual); 1 mark for describing antigenic shift (reassortment, novel subtype).
(c) [2 marks]
Antigenic shift poses a greater threat because it produces a completely new subtype of influenza virus against which the global human population has little or no pre-existing immunity (no memory cells or effective antibodies). This means the virus can spread rapidly across the world, causing a pandemic. In contrast, antigenic drift produces only minor changes, so some cross-protection from previous immunity usually remains, limiting the scale of outbreaks to seasonal epidemics.
Marking: 1 mark for novel subtype with no pre-existing immunity; 1 mark for pandemic potential / contrast with drift.
19. [7 marks]
(a) [2 marks]
As the concentration of bacterial toxin increases, the rate of cell growth decreases. At 0 μg/mL (control), cells grow normally from 10 to 80 ×10³ over 48 hours. At 5 μg/mL, growth is reduced (reaching ~50 ×10³). At 10 μg/mL, growth is minimal (~25 ×10³). At 20 μg/mL, the number of viable cells actually declines from 10 to 5 ×10³, indicating that the toxin is killing cells at this concentration. The effect is dose-dependent — higher toxin concentration produces a greater inhibitory effect.
Marking: 1 mark for describing reduced growth with increasing concentration; 1 mark for noting cell death at highest concentration / dose-dependent effect.
(b) [2 marks]
The bacterial toxin could inhibit cell growth by:
- Inhibiting protein synthesis — the toxin may inactivate ribosomes or modify elongation factors (e.g., like diphtheria toxin which ADP-ribosylates elongation factor 2), preventing the cell from producing essential proteins needed for growth and division.
- Damaging the cell membrane — the toxin could form pores in the plasma membrane, disrupting the cell's ability to maintain homeostasis, leading to cell lysis.
- Inhibiting DNA replication — the toxin could interfere with enzymes involved in DNA synthesis, preventing cell division.
Marking: 1 mark for a plausible mechanism; 1 mark for explaining how it affects cell growth.
(c) [3 marks]
The innate immune system would respond as follows:
- Phagocytes (neutrophils and macrophages) would be recruited to the site of infection by chemotaxis (following chemical signals such as histamine and cytokines released by damaged cells and resident macrophages). They would engulf and destroy bacteria through phagocytosis.
- The inflammatory response would be triggered: damaged cells and mast cells release histamine, causing vasodilation and increased capillary permeability. This increases blood flow to the area (causing redness and heat) and allows phagocytes and plasma proteins to move into the tissue more easily.
- Natural killer (NK) cells would be activated to destroy any host cells that have been infected by intracellular bacteria.
- The complement system may be activated, leading to opsonisation of bacteria (enhancing phagocytosis), inflammation, and direct lysis of bacterial cells via the membrane attack complex.
Marking: 1 mark for phagocytosis by neutrophils/macrophages; 1 mark for inflammatory response (histamine, vasodilation, increased permeability); 1 mark for NK cells or complement system.
20. [8 marks]
Model answer / Marking descriptors:
The human body is protected against infectious disease by two complementary arms of the immune system: non-specific (innate) immunity and specific (adaptive) immunity.
Non-specific (innate) immunity provides immediate, general defence against all pathogens. It includes:
- Physical barriers: The skin (keratinised epithelium) prevents pathogen entry. Mucous membranes in the respiratory and digestive tracts secrete mucus to trap pathogens. Cilia sweep mucus upward.
- Chemical barriers: Lysozyme in tears and saliva breaks down bacterial cell walls. Hydrochloric acid in the stomach kills most ingested pathogens.
- Cellular defences: Phagocytes (neutrophils and macrophages) engulf and destroy pathogens through phagocytosis. Natural killer (NK) cells destroy virus-infected cells and tumour cells by inducing apoptosis.
- Inflammatory response: When tissue is damaged, mast cells release histamine, causing vasodilation and increased capillary permeability. This brings more blood, phagocytes, and clotting factors to the site of infection.
- Complement system: A group of plasma proteins that can be activated to opsonise pathogens, attract phagocytes, and directly lyse bacteria via the membrane attack complex (MAC).
Specific (adaptive) immunity provides a targeted response to specific antigens and generates immunological memory. It includes:
- Cell-mediated immunity: Cytotoxic T-lymphocytes (CD8⁺ T-cells) recognise and destroy infected host cells by releasing perforin (which forms pores in the target cell membrane) and granzymes (which trigger apoptosis). Helper T-lymphocytes (CD4⁺ T-cells) coordinate the immune response by secreting cytokines that activate B-cells, cytotoxic T-cells, and macrophages.
- Humoral immunity: B-lymphocytes recognise specific antigens via their B-cell receptors. When activated (with help from helper T-cells), B-cells undergo clonal expansion and differentiate into plasma cells that secrete antibodies (immunoglobulins). Antibodies neutralise pathogens, opsonise them for phagocytosis, and activate the complement system.
- Immunological memory: After the primary response, memory B-cells and memory T-cells persist. Upon re-exposure to the same pathogen, they mount a faster, stronger secondary immune response, which is the basis of vaccination.
Integration: The innate and adaptive systems work together. For example, macrophages act as antigen-presenting cells (APCs): after phagocytosing a pathogen, they present antigen fragments on MHC class II molecules to helper T-cells, linking innate and adaptive immunity. The complement system enhances both innate (direct lysis) and adaptive (opsonisation for B-cell activation) responses.
Marking descriptors (8 marks):
- 1 mark: Description of physical/chemical barriers (skin, mucus, lysozyme, etc.)
- 1 mark: Description of phagocytosis (neutrophils/macrophages)
- 1 mark: Description of inflammatory response (histamine, vasodilation)
- 1 mark: Description of cell-mediated immunity (cytotoxic T-cells, helper T-cells)
- 1 mark: Description of humoral immunity (B-cells, plasma cells, antibodies)
- 1 mark: Description of immunological memory (memory cells, secondary response)
- 1 mark: Integration of innate and adaptive systems (e.g., antigen presentation)
- 1 mark: Quality of written communication — clear, well-structured, use of correct biological terminology
END OF ANSWER KEY
Free quiz and exam paper access
Enter your details to view this paper
Your access is remembered on this device.